As someone who has derived a surprising amount of blog traffic from posting about weight loss, I feel like I really ought to say something about Alas, A Blog’s case against dieting (which I first noticed via a Dave Munger comment). It’s a comprehensive collection of data (with graphs, so it must be Science) used to argue that the current weight-loss mania is all a bunch of crap, summarized thusly:
1) No weight-loss diet has every been scientifically shown to produce substantial long-term weight loss in any but a tiny minority of dieters.
2) Whether or not a weight-loss diet “works,” people who go on weight-loss diets are likely to die sooner than those who maintain a steady weight or who slowly gain weight.
3) For fat people (or anyone else) concerned with their health, the best option is probably moderate exercise and eating fruits and veggies, without concern for waistlines. In other words, Health At Every Size (HAES).
4) The model on which most weight-loss diets are based – in which fat people eat like fat people and must learn to eat like non-fat people – is probably a myth.
So, what’s the real story here? Is this just delusion spinning by a bunch of lard buckets, or is Jenny Craig a bigger mass-murderer than Pol Pot?
(Continued below the fold…)
I often think I’m doomed to remain a C-list blogger by the fact that I’m just too moderate to dedicate myself to posting ideological red meat. Much as I despise our Republican overlords, I can’t see myself as a hard-core Democratic partisan in the Kos mode; while I’m personally irreligious, I find hard-core atheists almost as hard to stomach as religious fanatics; and when the chips are down, I can’t even pick them back up to vigorously advocate fat acceptance.
I think a lot of what’s written in the Alas, A Blog post is more appealing than the weight-loss orthodoxy, both on personal (I can eat what I want!) and scientific grounds– a lot of the case for an “obesity epidemic” has always seemed like crap to me. I can’t really commit to either extreme, though– as with most science involving whole organisms (or, really, molecules more complicated than diatomics), I suspect the truth is messier, and somewhere between either of the convenient extremes.
This is also a nice illustration of the problems inherent in trying to make public policy on the basis of science that is necessarily incomplete– not only do you have the usual tensions within the scientific community, with different groups advocating their favorite models, but you also get huge political lobbies built up around the question. Even when you’ve probably overexaggerated the problems of “obesity,” you wind up with strong political pressure to not only not loosen current standards, but even make them more strict. It’s a big mess, which is why I don’t want to work with anything more complicated than diatomic molecules…
Anyway, I haven’t read the volumes of research material on either side of this question, but here’s my personal and idiosyncratic take on the whole issue:
Anti-Weight-Loss: Using online BMI calculators, the upper end of the “normal” range for somebody of my height is about 215 lbs, and the ideal range would be more like 190 lbs (do your own metric conversions). To put this in perspective, I weighed about 190 when I was a senior in high school, playing three sports. In basketball season, I was playing hoops for two to three hours a day, six days a week.
There’s a picture of me from my high school graduation hanging on the wall in my parents’ house. The first time Kate saw it, she started giggling uncontrollably. I look ridiculous at that weight, and maintaining it, even back then, was extremely difficult. (When I went away to college and started playing rugby, I jumped up to 240 lbs within a year or so, and was much more comfortable.)
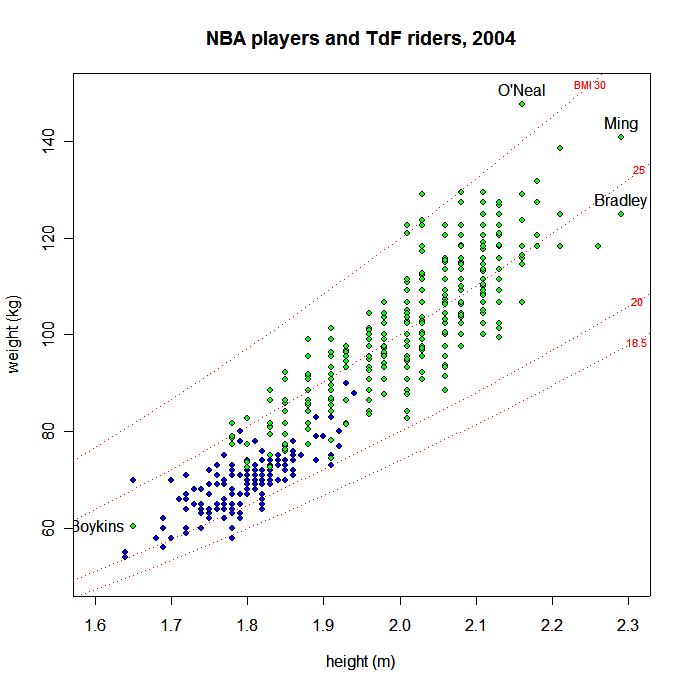
Particularly for tall people, the standards set by the BMI have always struck me as absurd, and they’ve only gotten worse over the years (I think the lowering of the levels is a significant factor in the “obesity epidemic”– people are classified as overweight or obsese who used to fall into the normal range, under the old standards. They haven’t gotten any fatter or less healthy, it’s just the standard that has changed). There’s clearly something a bit off in those standards when, as a commenter pointed out in my earlier post, large numbers of NBA players are technically “obese.” (Spiffy graphic here.
{kind=link}
The responses to any evidence that appears to contradict the standards is also telling. The MSNBC article cites “experts” as saying that the “obese” classification is justified because “athletes tend to keep their high BMI’s after they retire.” That’s a nice little trick, right there– because you’re going to be fat in the future, it’s OK to call you fat now. I’m going to be dead in the future– does that make me a corpse?
I also liked the response to to meta-study a few years back showing that people with slightly higher BMI had a slightly longer life expectancy than people in the “normal” range. The news stories reporting it were full of complicated justifications about fat cushioning falls and so on, while the simplest explanation– the current “normal” range is both too low and too narrow– was neve brought up. This is no way to conduct science.
Pro-Weight-Loss: I felt that way before I ever saw the Alas, A Blog compendium of fat-positive research. So why did I set out to lose weight earlier this year?
It was a combination of things, really, but in the end, it came down to this: I’m 34– climbing three flights of stairs shouldn’t leave me gasping for breath. I decided to lose some weight because I was eating too much and not exercising enough. My knees hurt when I played basketball, and I would get light-headed if I stood up quickly. (Also, some asshole doctor told me that my reflux problems would go away forever if I lost weight… It’s going to take a real effort not to slug him the next time I see him.)
I complained in that last post about my energy levels and so on after my recent dramatic weight loss, but really, the first ten pounds or so were a clear positive– I felt better all the way around. And even now, some things are clearly improved by carrying around less weight– my knees don’t hurt as much, my lower back isn’t giving me as much trouble, and I can climb stairs without gasping (unless I take them two at a time). When my stomach is calm enough to eat a reasonably normal diet, I even feel reasonably good on the energy level front.
And, prior to the stomach issues, this did not require a drastic lifestyle modification– I played a little more basketball (and made an effort to run the break more often), took the stairs, and stopped eating junk food at work. This wasn’t a crash diet, and didn’t involve becoming a fitness freak.
I think that, while the official standards are ludicrous, I was definitely overweight at 280, and I knew it (even though I probably would’ve classed myself as “healthy” there). 190 is completely ridiculous, but 240-250 is prefectly reasonable, and I’ll probably try to maintain that level even after the stomach thing gets sorted out.
So that’s my take, for whatever it’s worth. I’d love to have some brilliant and insightful summation, but I need to go teach, so I’ll leave off here before I start to sound like one of those tedious fitness Nazis promoting a weight loss scheme on late-night cable.
I have not looked at the studies in question, but I have some doubts. For example, the blog says studies have not found that fat people consume more calories and burn fewer than thin people. Even assuming some differences in efficiency of metabolism, how can that be physically justified? Do the thin people have a higher body temperature? Human bodies do not violate normal physical laws. I would also like to see how the reported death rates for “thin” people square with the animal studies that appear to show an increased life span associated with reduced calorie intake.
But is there an obesity epidemic in the US? Of course not; that’s just TV talk. It’s absurd to call a national weight problem an epidemic, as if it were contagious. But when I look around, I see a hell of a lot of fat people, including children. When I look at my 1st grade class picture (from the mid-50s) there are only about two or three kids out of about 30 that look overweight. I have a hard time believing fat kids are bound for a long, healthy life. I presume the weight is a symptom of the real problems, which include eating lots of junk food and getting little or no exercise. I doubt that diets are the solution for kids, but a little parental control over junk food and a little normal exercise sounds like a good idea.
Your first link is broken.
Nice post. I went from BMI 32.1 to BMI 25.7 over the past year for most of the same reasons you give (though I don’t have reflux, my doc was threatening to put me on blood pressure meds full time.) The change in weight was primarily due to going from a fairly sedentary lifestyle to running 20-30 miles per week and secondarily from making shifts in the foods that I eat daily. I did not give up good food since I like most food anyway, just made a conscious effort to have one more serving of broccoli before having seconds on the pasta and bringing my lunch to work — that kind of thing. I still have steak/lamb on a regular basis (OK, now weekly rather than twice a week) and real ice cream.
Anyhow, at BMI 25.7 the wife said I’m looking gaunt and told me she was going to start subing whole milk into my fat-free container if I lost any more weight so I upped my calories a touch and started exercising the upper body a bit. One of these days I may drop into the “normal” range just to see what it feels like, but for now I’m comfortable at 26.3. Honestly, though, I agree — the BMI normal range is ridiculously narrow.
Seems to me there are two different issues here:
1) Is losing and maintaining weight in a healthy way a net win for obese people?
2) If 1) is true in theory, in practice does the likelihood of successful weight loss in our society outweigh the risks of gain-loss cycles?
No answers from me, but two other points:
1) I’d thought that those studies claiming that obese and lean patients consume similar numbers of calories are based on self-reported data, and that when you get hard numbers (from monitored patients or isotope tagging) it turns out that the obese do eat more.
2) The athlete issue seems a red herring. Even beyond the fact that there probably are four genuinely obese players in the NBA, and certainly are many in the NFL, that a guideline breaks down in extreme outliers doesn’t mean it’s not generally informative.
It could be that the BMI is designed to give false positives. Better you talk to a doctor, or rethink your exercise regimen, or whatnot and discover that you’re ok than have a heart attack. Also, in addition to breaking down for tall people, it doesn’t do a good job (especially since it isn’t trying) to account for torso size – two people the same height with radically different inseams and shoulder breadth will calculate the same BMI. As for whether diets work or not, it probably depends on how you judge compliance and whether to count exdieters as dieters (they started the program and it didn’t help) or nondieters (they weren’t following the guidelines, after all). I also would wonder whether the over alarm is deliberate because there is a little backsliding built in – if we say exercise for 1 hr/day they’ll actually exercise for 30 min/every other day, which is the actual goal.
The BMI standards (assuming that the online calculator link implements them correctly) are whacked.
If they are correct, I would have been considered “overweight” (26.1 BMI) when I was in the Army in peak physical condition.
I weighed *177*. I didn’t look like a bodybuilder. I didn’t look like a powerlifter. I looked like a 22 year old, 5’9″ guy in decent shape. I could do 90 pushups, 90 situps, and run 2 miles in about 10:30 — maxing the Army’s PT test. Yet the BMI says I was overweight.
Seriously, WTF? People buy into these standards?
That at least is easy enough to explain. An increased life span is only associated with certain reduced calorie diets. (And thinness is not quite the same thing as “on a reduced-calorie diet”). And the effect is largest when you reduce the calorie intake past “thin” and into “gaunt” territory. Which is a dangerous thing to do unless you really know what you’re doing. I don’t, so I wouldn’t attempt it.
Even the medical community is ready to admit that Body Mass Index as calculated by a height/weight chart offers a less than ideal measure of well being. The current research has most considering a waist-to-height ratio as a better alternative. That first ten pounds off is reportedly principally comprised of interstitial fat; the fat that surrounds the internal organs which is considered the most damaging to health. Getting off the first ten does tend to make people feel a whole lot better as a result. The rest comes off proportionately according to some individually determined DNA dynamic (which I have yet to figure out). As a female I’m distressed that I can’t make the excess inches come off my hips *before* it comes off my chest! Anyway, athletes (and, determined recreational fitness folks) may be particularly poorly served by standard BMI calculations. I’ve been told that it is true; cubic centimeter for cubic centimeter, muscle weighs more than fat. If you’re building muscle but losing inches off your waist, the bathroom scale may not adequately reflect that change.
BMI was designed to be easy to calculate rather than accurate – it’s the medical equivalent of teaching mechanics with algebra because calculus is too complicated – or worse. As such, it shouldn’t really be surprising that an approximation breaks down three sigmas out (6’6″ might even be more than that).
Bodyfat percentage is much more directly relevant, and I’m pretty sure that someone in the athletic department would be willing to whip out the skin-fold calipers and give you a number.
Brian Ledford: It could be that the BMI is designed to give false positives. Better you talk to a doctor, or rethink your exercise regimen, or whatnot and discover that you’re ok than have a heart attack.
I think there’s probably some element of that.
The problem with that idea is the same as the problem with a lot of anti-drug scare tactics. You could argue that telling kids that smoking even a little marijuana leads inevitably to living out in the trash giving hand jobs for crack will scare them enough that they’ll be more cautious about experimenting with pot, which actually isn’t all that bad. The problem with that theory is that they’re equally likely to smoke one joint, realize you were lying, and assume that the warnings about more dangerous drugs were also horseshit.
I wonder how the number of people scared into early doctor visits by unrealistic BMI standards compares to the number of people who see the unrealistic standards, and decide that the medical community is dipping a little too deep into the pharmaceutical stocks in their off hours, and stop paying any attention. Or even worse– I only glanced at the comments to the Alas, A Blog post (the link should be fixed shortly after I post this), but there seemed to be some real conspiracy-theory stuff in there.
It would shock me if collegiate gymnasiums did not have a handful of those handheld electronic body fat percentage indicators, or even one of the step scale ones.
As far as I can figure, they pulse either low level RF or ultrasound and measure the returns, then index against your weight. (What I’ve read indicates RF, but I’ve never seen one warn people with pacemakers about it, and frankly, ultrasound just plain makes more sense.) They’re supposed to be relatively accurate, which would be enough for any casual dietter and most amateur athletes. I’ve used one a few times at the health club, and at the very least they hold up to sanity checks of the, “Well, I lost this much weight, and it was all cardio, so it was probably mostly fat and not much muscle gain, which would mean blah blah blah…” sort.
On the subejct of intentionally misleading BMI charts, first, I don’t give the vaunted “community” that much credit for forethought, and second, there’s also the risk of people who are already doctor-averse just deciding not to go because they can’t handle the bad news. I have several of those types in my family. Hell, it could be it’s just a bad metric that even physicians of the sort who make physics teachers cringe in horror can still grind through or look up on a chart.
The electronic ones are certainly easier to use and are reasonably precise, but they are very sensitive to your state of hydration. Even more so than your weight.
But yes, they’re worlds better than BMI.
What a coincidence. Slate has one of Saletan’s “science” posts and it mentions some studies on this issue:
http://www.slate.com/id/2139169/
BMI is useless when folks have significant muscle mass. It’s simply a calculation using weight and height, a quick rule of thumb. It works O.K. with most relatively sedentary people, but its uses are limited.
Percent body fat is much more helpful, but is tricky to measure accurately.
“Normal” systolic blood pressure has been dropped 10 torr to 130. “Normal” cholesterol levels are suggested for maintenance in children. Using Enviro-whiner rules of engagement, by the year 2250 when the whole planet spontaneously combusts from Global Warming we will have blood pressures of 60/45 and no cholesterol at all in our bodies – especially not in our brains that are a historical ruinous 30 wt-% cholesterol.
One anticipates Official whining about ear wax or farts (especially in the Los Angeles basin), massively funded studies thereafter, and a rash of pharmaceuticals to remediate the problem (followed by a side effect scandal or two). We cannot, will not stop at Restless Leg Syndrome, oh no!
I realize that was a joke, but as someone who’s experienced sensations very much like a mild form of Restless Leg Syndrome–even that is hideous. If someone else were doing it to me, I’d call it torture.
Actually, in a very rare moment of hypochondria, the first time I saw a commercial for whatever drug is supposed to help RLS, I stared at the screen and thought, “Oh. Is that what that is?”
I must remember to find out if there’s a reliable screening procedure for that because, while I am almost always fidgetting with my feet and legs, there is such a thing as just being restless and hopped up on too much coffee.
For fat people (or anyone else) concerned with their health, the best option is probably moderate exercise and eating fruits and veggies, without concern for waistlines. In other words, Health At Every Size (HAES).
Tell it to people who had got obesity-induced diabetes. (Excess fat produces excess insuline).
I’m in the normal range according to your BMI calculator, but at the top end. To be in the middle for my height (5’7″), I’d have to get down to 140lbs. I haven’t weighed 140 since I was 20, and I looked like a potential famine victim when I did (which is because I was, since I couldn’t always afford to eat every day at that point). I was not healthy at 215, but 155 is damn comfy and easy to maintain.
My guess is that longevity under laboratory animal conditions and longevity in the wild are very different things. Mouse labs are clean, almost aseptic. I can easily believe that reduced calorie intake produces vulnerability that is masked in the lab but causes mortality in the wild.
I’m smack in the middle, 21.6. But I’m also always described as “that skinny guy over there.” I’ve been trying to work out more lately, including walking or biking to work and jogging regularly. I’m clearly not concerned with weight, but I am concerned about production of bad cholesterol and general cardio health. (I also avoid the car to save my money and the environment. Cheap and generous at the same time, enough to impress the most depressed robot.)
I notice that, assuming his posse has his stats correct, John Lynch has a BMI of 23.1.
I think the BMI reading being low can be dangerous. My whole family is tall, with me at 6’1 and my sister about 5’9″. My sister is constantly underweight from not eating, but because she is barely within her BMI her doctor always tells her she is fine. Sometimes when I see her, she is just skin and bones, and I can see her hips stick out. I can’t believe that is healthy. So, for people like her, I think a false positive is a bad influence on her health. It just convinces her she should continue with her habits.
Slate article: “calorie restriction might slow the break down of DNA that occurs as animals show the effects of aging.”
“Doctor, doctor, it hurts when I do this.”
“Don’t do that.”
The joke is funny, because a real doctor would try to find the source of the pain, and come up with an effective treatment.
Blaming obesity on lifestyle (diet and exercise) is a lot like that old joke. Just as pain is real, hunger is real, and lethargy is real. I eat when I’m hungry; I rest when I’m tired. I don’t eat when I’m not hungry, and I don’t rest when I’m not tired. Thin people are no different from me in that regard. Telling an obese person to eat less and exercise more is absolutely fucking useless, medically. It’s as willful a denial of observable reality as young-earth creationism or flat-earthism.
The notion that obesity is caused by voluntary lifestyle choices is a very attractive one. It plays into all kinds of prejudices, guilts, and fears, and allows the non-obese to engage in an orgy of smarmy self-congratulation. It reflects the worst kind of confirmation bias, and has no place in science or medicine.
[/rant]
Umm… I may be sticking my nose in, but I feel so awful for you. Reflux is no fun at all. I am probably going to sound like a moron, whoo hoo freaky one, but I was wondering have you ever tried lactobacillus acidophilus??? In capsule form. Not scientific and only anecdotal, but when I have had reflux it is the only thing that has helped. I am not a doctor, obviously, so check it out yourself, and I really hope that SOMETHING helps. (PS_ When I got a case of C Difficile it was what helped make life bearable- and there are studies out of Europe that purport that to be true as well. ) Get better- you are way to young to be in pain.
Check with a doctor of course, and PLEASE know that I am not a whoo hoo weirdo…..I promise. I go to real doctors, have never done a faith healing, gone to chiro, visited a naturopath or taken a homeopathic remedy etc….